Electrocardiogram 3: cardiac rhythm and conduction abnormalities - Nursing Times
The last of three articles on using an electrocardiogram to assess the heart's electrical activity focuses on causes of cardiac rhythm and conduction abnormalities and how to spot them
Abstract
This is the last in a three-part series on using an electrocardiogram to assess the heart's electrical activity. In this article, the focus is on cardiac rhythm and conduction abnormalities of the heart, which all have unique presenting characteristics. These characteristics include ectopic beats, tachycardias and atrioventricular block.
Citation: Jarvis S (2021) Electrocardiogram 3: cardiac rhythm and conduction abnormalities. Nursing Times [online]; 117: 8, 27-32.
Author: Selina Jarvis is honorary research nurse, Guy's and St Thomas' NHS Foundation Trust.
- This article has been double-blind peer reviewed
- Scroll down to read the article or download a print-friendly PDF here (if the PDF fails to fully download please try again using a different browser)
- Click here to see other articles in this series
Introduction
This is the final article in a three-part series on use of an electrocardiogram (ECG), a non-invasive and quick investigation that assesses the electrical activity of the heart. Part 1 looked at the purpose of the test, cardiac electrophysiology and the practicalities of doing an ECG, while part 2 looked at interpretation, with a particular focus on cardiac ischaemia. In this article, the focus is on abnormalities in rhythm and electrical conduction that can be identified on an ECG.
Cardiac arrhythmias and conduction defects are common. They can be an acute problem presenting for the first time, or part of a chronic disease course complicated by acute decompensation at periods of illness. Some arrhythmias may cause little to no symptoms and are fairly benign, while others are of greater concern and may lead to serious symptoms; at worst, they may predate a cardiac arrest if not recognised and treated promptly.
Clinical assessment of arrhythmia
The following steps are key when assessing a patient presenting with an abnormal heart rhythm or conduction defect:
- Take a history of the complaint/symptom with which the patient presents;
- Consider whether there are any features of cardiac compromise (specifically, shock, syncope or fainting, myocardial ischaemia, heart failure);
- Consider any relevant past medical history;
- Take note of medications that may be associated with the condition;
- Ask about family history of arrhythmias, cardiac disease or sudden cardiac death;
- Consider relevant investigations, such as electrolyte abnormalities. Excess, or deficiencies in, potassium, magnesium or calcium can affect the balance of electrical charges inside and outside of cardiac cells, alter electrical signalling and cause arrhythmias;
- Compare with previous ECG results if available.
Clinical symptoms
There are various potential symptoms associated with an arrhythmia. One common symptom is palpitations but this can mean different things to different people. Some report it as an increased awareness of a heartbeat or fluttering in the chest, while others may report feeling an extra or missing beat or complain of an irregular heart rate. You can ask patients to tap out the rhythm of the beat they felt onto a table with their hands or show you their device if they have recorded an event.
Symptoms may also include dizziness or syncope. Syncope may be due to a simple faint, often when standing for a long period of time or when standing up from a sitting/recumbent position (postural) or at rest, and can be related to aberrations in heart rhythm or conduction defects. Be aware that there may be causes of a cardiogenic or neurogenic nature (for example, seizures) to consider in the differential diagnosis.
Other symptoms are increased breathlessness, sweating or chest pain; these signs may be more common with tachycardias (see below). With the advent of fitness technology, such as smart watches, some patients may present with or without a history of symptoms after identifying abnormal activity on their ECG mobile app.
Recognising cardiac arrhythmias
When considering whether cardiac rhythms are normal, it is important to understand the electrical conducting system of the heart and how the ECG works, which were covered in parts 1 and 2 of this series. In summary, the sinoatrial node (SAN) is the natural pacemaker of the heart, generating a signal without an external stimulus. If this stops working, other slower potential pacemakers in the heart, such as the atrioventricular node (AVN) or bundle of His, can take over (Jarvis and Saman, 2018). In these circumstances, overall heart rate will be slower.
The key components of the cardiac conducting system are discussed below and listed with their usual intrinsic rates in Table 1.

Ectopic beats
Ectopic beats are common and characterised by single electrical impulses that originate away from the SAN as extra beats. They are generally benign and of no clinical significance. In the presence of an atrial ectopic (premature atrial contraction), an extra wave is seen within the P-wave (atrial depolarisation) so it looks different to normal on the ECG. Ventricular ectopic beats (premature ventricular contractions) look more dramatic, with a:
- Large wave on the rhythm trace typically not preceded by a P-wave;
- Wide overall QRS complex (ventricular depolarisation) of more than 120 milliseconds (ms) and inverted T-wave (ventricular repolarisation) (Fig 1).

If there are isolated ectopic beats, there is likely to be little clinical significance or action needed (Omar et al, 2011). However sometimes there is a ventricular ectopic beat after every normal QRS complex; this is referred to as ventricular bigeminy and suggests some ventricular irritability.
If the patient is symptomatic with frequent ectopic beats, make sure you ask them about potential medications that can interfere with heart rate (for example, salbutamol, digoxin, over-the-counter cold and allergy drugs, or antiarrhythmic drugs), as well as high caffeine and alcohol consumption. Further investigations may be needed, such as checking electrolytes (potassium, magnesium and calcium) and thyroid function and, sometimes, a 24-hour or 48-hour Holter monitor or ECG may be required.
Sinus bradycardia
Sinus bradycardia is a slow heart rate of ≤60 beats per minute (bpm), due to the slowing down of the SAN. This may be physiological, often occurring in fit individuals like athletes, and may be related to an increase in the vagal tone of the heart caused by the vagus nerve (actually a group of nerves that control parasympathetic activity in the heart). Bradycardia can also be caused by vomiting, straining (through vagal effects), beta-blocker drugs and raised intracranial pressure from head injury/pathology. It can also happen in the context of an inferior myocardial infarction in which the SAN is in the region supplied by an occluded coronary artery — usually, the right coronary artery affecting the sinoatrial artery.
Bradycardia can be caused by diseases such as sick sinus syndrome, when there is an irreversible dysfunction of the SAN that affects its ability to generate electrical impulses to the heart. This can cause a pause in electrical signals from the sinus (lasting seconds to minutes), or electrical impulses for which signals from the sinus are slow or blocked. The dysfunction can result in an alternating slow and fast heart rate called bradycardia-tachycardia syndrome, or there may be atrioventricular block (described later in this piece). When there are symptoms due to sinus node problems, the patient may need to have a pacemaker inserted (National Institute for Health and Care Excellence, 2014a).
"It is important to keep an open mind to the potential causes and take a proper clinical history"
Sinus tachycardia
In sinus tachycardia, the SAN is firing at a rate of ≥100bpm, but the rest of the conducting system is normal. There are many benign causes, such as sinus tachycardia in response to pain or exercise, as an adaptation in pregnancy, a response to caffeine or a side-effect of medications such as salbutamol or digoxin.
Sinus tachycardia can also occur with fever, infection, dehydration, electrolyte (typically calcium, magnesium or potassium) abnormalities, and overactive thyroid. However, it can signify more-dangerous conditions, such as pulmonary embolism, and it is important to keep an open mind to the potential causes and take a proper clinical history.
Assessing tachycardias
A normal heart rate is 60-100bpm; tachycardia refers to a fast heart rate of >100bpm. It has different causes and the reason for the fast heart rate can originate from the atria or the ventricles. Tachycardia may be transient, lasting for seconds or minutes, but can also last for several days.
It is possible to differentiate between tachycardias that originate in the atria or ventricles by looking at the width of the QRS complex, which is normally 120ms. In tachycardia originating in the atria (supraventricular), the QRS is typically narrow (<120ms) compared with that originating in the ventricles (ventricular tachycardia), for which the QRS is broad (≥120ms).
Supraventricular tachycardia
Supraventricular tachycardia, with the characteristic narrow QRS complex, may originate in the atria or AVN. There are many different causes, including known cardiac or lung disease, particular medications, substance misuse, smoking, infection and pregnancy. The interpretation of an ECG should be done in a methodical way (Jarvis, 2021a). For tachycardia specifically, you should consider whether:
- There are any P-waves;
- The rhythm looks regular or irregular;
- It is narrow or broad complex tachycardia based on the duration of the QRS complex (Ganz, 2019).
The most common sustained narrow complex tachycardia is atrial fibrillation (AF) (NICE, 2014b). There are several causes (Table 2) and a steep rise in prevalence with age. In AF, the atria have many mini circuits originating from small islets due to atrial remodelling. As a result, there is chaotic electrical activity with no concerted atrial depolarisation, which leads to an irregular, fast heart rhythm. As the electrical activity does not originate in the usual way from the SAN, there is a lack of P-waves and the rhythm strip of the ECG looks irregular (Fig 2a).


AF can spontaneously revert back to sinus rhythm or resolve once the underlying cause has been treated but the longer patients have the condition, the less likely it is to terminate spontaneously; they will need medications for rate control and anticoagulation due to the risk of clots forming in the fibrillating atria (Olshansky and Arora, 2019). As AF increases stroke risk by up to five times, it is crucial to consider anticoagulation based on a scoring system.
Atrial flutter – the causes and ECG features for which are outlined in Table 2 – is a supraventricular tachycardia that is regular, but the atrial rate is up to 300bpm and there are flutter waves that form a continuous sawtooth line. Although the atrial rate is 300bpm, the AVN has a delay due to its slower intrinsic rate so it is not able to transmit this fast rate and slows down atrial flutter typically to around 150bpm (Olshansky and Arora, 2019). This is a protective mechanism to prevent the impulses being transmitted into the ventricles. The result on the ECG is sawtooth-looking waves, instead of normal P-waves; not all of these are followed by a QRS complex so there are sometimes two P-sawtooth-waves preceding a QRS, which is referred to as a 2:1 block (Fig 2b).
Another narrow complex tachycardia that can occur at any age is atrioventricular-nodal re-entrant tachycardia (AVNRT), a common cause of paroxysmal supraventricular tachycardia caused by the formation of a re-entry circuit in the AVN or tissue around it (Knight, 2020). It develops suddenly, often with concomitant sudden onset of palpitations, and can relate to underlying structural heart disease but is precipitated by stress, alcohol, caffeine and other stimulants. On the ECG, there is a regular, narrow complex tachycardia with a heart rate of 120-220bpm. Fig 2c shows supraventicular tachycardia, which is a common type of AVNRT.
Management includes vagal manoeuvres to slow the AVN, such as carotid sinus massage of the neck or asking the patient to blow into a 50ml syringe (if not contraindicated). Otherwise, pharmacological control may be needed with adenosine (3mg intravenously over two seconds (s), followed by 6mg after 1-2 minutes, if required, then 12mg after 1–2 minutes). This can slow down the heart rate and help to identify a regular tachycardia.
Paroxysmal supraventricular tachycardia can be a result of AVNRT but, in younger patients, can be due to Wolff Parkinson White syndrome, in which an accessory pathway linking atria and ventricles bypasses the AVN, and for which there is a characteristic delta wave present on the ECG (Chhabra et al, 2020). With any supraventricular tachycardias, if there are any adverse features, electrical or chemical cardioversion may be required to bring the patient back into sinus rhythm.
Ventricular tachycardia
This is a broad complex tachycardia originating in the ventricles with a heart rate of >100bpm and a QRS complex of >120ms. For the most part, a broad complex tachycardia is likely to be due to a ventricular tachycardia and it is safest to consider this first, given the urgency for treatment.
In some cases, the problem may originate in the atria, such as with AF when a defect of electrical impulses down the bundle branches results in an ECG suggestive of a broad complex tachycardia. In this case of AF with a bundle branch block, there would be an absence of P-waves and the rhythm would be irregular, along with the broad QRS complex. Looking at the QRS complex may also be helpful in ventricular tachycardia because the heart rate is regular and the QRS looks monomorphic (uniform) throughout the ECG trace.
It is crucial to recognise ventricular tachycardia on an ECG or cardiac monitor because it needs urgent medical attention; guidance on this can be found in the Resuscitation Council UK's guidelines by Soar et al (2021).
Depending on whether there are adverse features and signs of haemodynamic compromise, such as shock, syncope, or chest pain, electrical cardioversion may need to be considered to bring the heart back into sinus rhythm. Pharmacological agents are another option for rate control and treatments include beta-blockers, calcium channel blockers or chemical cardioversion with amiodarone.
In polymorphic ventricular tachycardia (Fig 3a), the shape of the QRS complexes look very different to monomorphic complexes (Fig 3b). In a condition called torsades de pointes, the broad complex QRS complexes are polymorphic and look to be twisting around the electrical baseline with prolongation of the QT interval (Fig 3a). Torsades de pointes is a dangerous heart rhythm that can lead to dizziness and syncope; in addition, although in some cases it may spontaneously revert to sinus rhythm, it can also lead to a cardiac arrest with ventricular fibrillation. After checking electrolyte levels and giving magnesium intravenously, if needed, electrical cardioversion may be required.

Causes of ventricular tachycardia and torsades de pointes are outlined in Table 2.
Conduction abnormalities
Conduction defects can be caused by problems at the level of the AVN or through the bundle of His and bundle branches.
Atrioventricular block
Atrioventricular (AV) block relates to a problem in conduction in, or in close proximity to, the AVN. When an electrical impulse leaves the atria and travels to the AVN, there is a delay which is represented by the PR interval (beginning of the P-wave to the start of the QRS complex) (Jarvis, 2021b). The maximum PR interval is 120-200ms (or three to five small squares of the ECG). If there is a delay in the PR interval, this is referred to as AV block or heart block of which there are key classes (Fig 4).
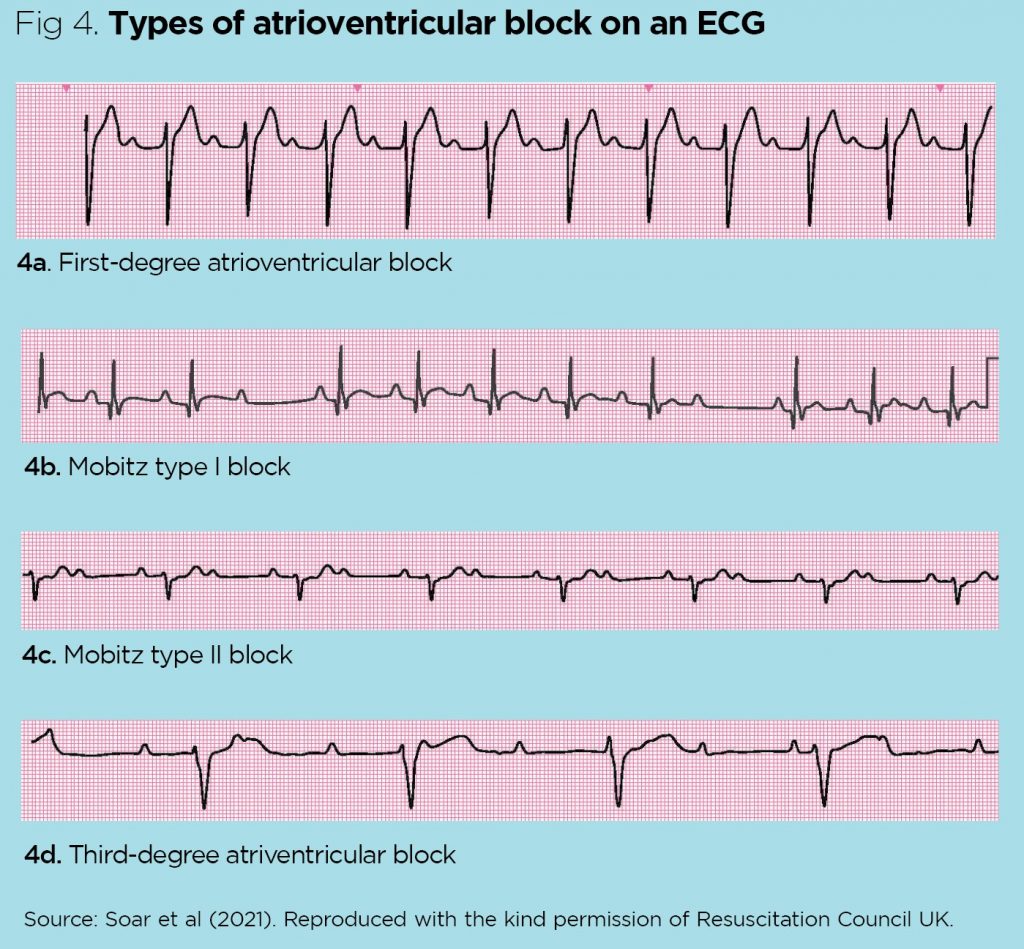
First-degree AV block (Fig 4a) is when there is a constant prolongation of the PR interval of ≥200ms. This is usually a benign state in which patients tend to be asymptomatic and it may not have been found had they not had an ECG.
There are two sub-types of the second-degree AV block: Mobitz type I and Mobitz type II. In both conditions, a P-wave is blocked from initiating a QRS complex. In Mobitz type I (also called Wenckebach), the disease is in the AVN; it is a more benign AV block than in Mobitz type II and can be identified by a prolonged PR interval, which progressively increases on successive beats until there is a dropped beat (Fig 4b).
This differs from Mobitz type II in which the problem is below the AVN (most likely in the bundle of His or Purkinje fibres) and, intermittently, a non-conducted P-wave can be seen (that is, there is no QRS complex). This can happen every other beat, referred to as 2:1 block (Fig 4c), or every third beat, referred to as 3:1 block. Mobitz type II is associated with a worse prognosis and can progress to third-degree heart block.
In third-degree AV block, there is an absence of conduction between the atria and ventricles, and a complete lack of relationship between the P-waves and QRS complexes (Fig 4d). In this case, the junctional cells found just before the bundle of His bifurcate into bundle branches and act as an escape pacemaker that takes over. This results in a heart rate of 40-60 bpm and is a serious condition with the risk of sudden loss of cardiac output. Avoiding those drugs that slow the AVN, correcting any electrolyte problems, giving atropine that blocks the vagal nerve (0.5mg intravenously every 3-5 minutes until a 3mg maximum dose is reached) can treat the AV block temporarily by bringing up the heart rate ready for urgent pacemaker insertion.
Table 3 summarises the differences in the ECG findings and causes of AV blocks.

Bundle branch blocks
In the normal heart at the level of the bundle of His, conducting fibres split into the right and left bundle branches, which conduct electrical impulses to the right and left ventricles, respectively. This impulse usually occurs in synchrony and the ventricles contract simultaneously. If there is a block in one of the bundle branches due to damage, there may be a delay in the electrical impulse leading to that ventricle, causing a widened QRS complex exceeding 120ms. In the case of the right bundle branch block (Fig 5a), this can happen because of normal variation or due to diseases such as atrial septal defect, pulmonary embolus or cor pulmonale (heart failure due to lung disease).

Left bundle branch block can be seen in healthy people, but is also due to various cardiomyopathies, hypertension and fibrosis of the heart (Hampton and Adlam, 2019). Most patients with a bundle branch block (Fig 5b) are stable and intervention is only needed if they become symptomatic.
Conclusion
A good knowledge of the conducting system of the heart, including appreciating that depolarisation begins in the SAN and the route of the electrical impulse, is useful when understanding and identifying conduction defects and arrhythmias. This series has covered the principles and practicalities of ECG and how to take a methodical approach to its interpretation, while considering potential causes in context of the clinical situation and medical history.
Key points
- Cardiac rhythm and conduction defects, such as atrial fibrillation, are common
- They can be an acute problem presenting for the first time or part of the course of a chronic disease
- When considering whether cardiac rhythms are normal, nurses need to understand the electrical conducting system of the heart
- A clinical history should include medicines and current symptoms when assessing rhythm disorders
- It is important to understand the unique patterns in rate and waveform on the electrocardiogram that are associated with different disorders
Also in this series
Chhabra L et al (2020) Wolff Parkinson White Syndrome. Treasure Island, FL: StatPearls Publishing.
Ganz LI (2019) Wide QRS complex tachycardias: approach to diagnosis. UptoDate.com, 4 November.
Hampton JR, Adlam D (2019) The ECG Made Practical. Elsevier.
Jarvis S (2021a) Electrocardiogram 2: interpretation and signs of heart disease. Nursing Times; 117: 7, 54-57.
Jarvis S (2021b) Electrocardiogram 1: purpose, physiology and practicalities. Nursing Times; 117:
6, 24-28.
Jarvis S, Saman S (2018) Cardiac system 1: anatomy and physiology. Nursing Times [online]; 114: 2, 34-37.
Knight BP (2020) Atrioventricular nodal reentrant tachycardia. UptoDate.com, 26 October.
National Institute for Health and Care Excellence (2014a) Dual-chamber Pacemakers for
Symptomatic Bradycardia due to Sick Sinus Syndrome without Atrioventricular Block. NICE.
National Institute for Health and Care Excellence (2014b) Atrial Fibrillation: Management. NICE.
Olshansky B, Arora R (2019) Mechanisms of atrial fibrillation. UptoDate.com, 22 October.
Omar AR et al (2011) Managing ventricular ectopics: are ventricular ectopic beats just an annoyance? Singapore Medical Journal; 52: 10, 707–713.
Soar J et al (2021) Adult Advanced Life Support: Guidelines. Resuscitation Council UK.
Electrocardiogram 3: cardiac rhythm and conduction abnormalities - Nursing Times


Comments
Post a Comment